Aphasia
|
|
Aphasia is a speech and language disorder that can result from traumatic brain injury, and one that greatly affects the bilingual community. It generally occurs from a legion to the language dominant side of the brain and results in difficulty with language production or processing. The aphasias listed below are the most common to result from TBI and the most commonly seen by practicing speech-language pathologists.
|
Broca's AphasiaBroca’s aphasia, or expressive (non-fluent) aphasia, occurs accompanying a traumatic lesion to the frontal and usually left lobe of the brain. As a result, the patient is unable to form fluent speech, or unable to do so without extreme difficulty. The disorder is categorized as nonfluent, with decreased verbal output, decreased phrase length, agrammatism, and dysprosody (referring to the natural rhythm and patterns of speech) (Cummings & Mega, 2003).
Some aspects of literacy are affected, including the ability to read aloud, the ability to write, and the ability to repeat written words. The severity of the lesion to the brain generally affects the severity of the aphasia, as does the location of the lesion. For example, damage to the Broca’s area and the frontal operculum, which contains nerves of the tongue, can result in difficulty initiating speech. Lesions including injury to the lower motor cortex can result in dysarthria, a disorder that limits the muscle movement required to make speech that results in slurred speech. Both Broca’s and Wernicke’s aphasias have an “overall fair” prospect of recovery with the help of speech and language therapy, but cases vary based upon the individual (Cummings & Mega, 2003). |

A lesion to Broca's area
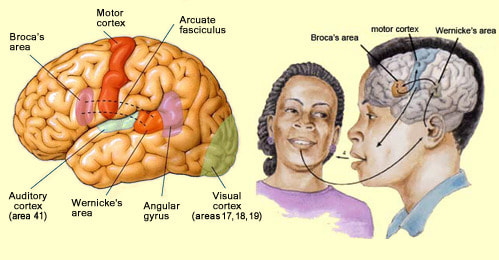
A demonstration of a normally functioning Broca's area. In Broca's aphasia, the connection to the motor cortex is impaired and the subject is unable to produce fluent speech. Image courtesy of https://www.thinglink.com/scene/886029669311184896
|
Wernicke's Aphasia |
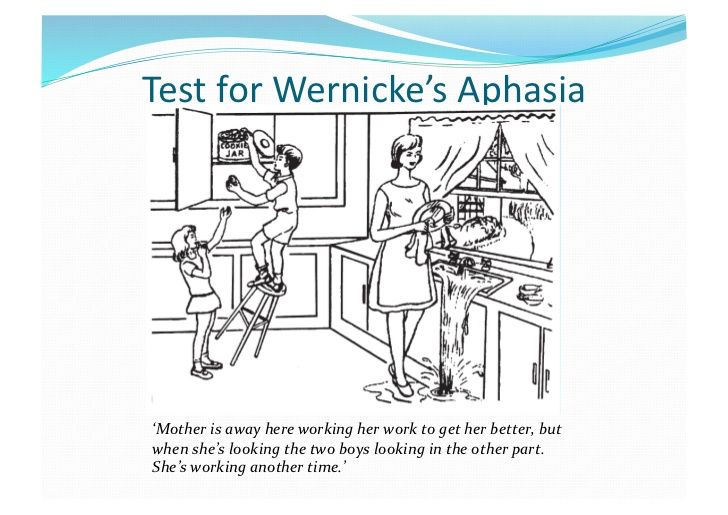
A common test for Wernicke's aphasia is to show a patient this cartoon and ask them what is going on in the picture. The dialogue is a potential response by a subject with Wernicke's aphasia. Image courtesy of https://www.slideshare.net/coburgpsych/lesson-7-brocas-aphasia-and-wernickes-aphasia
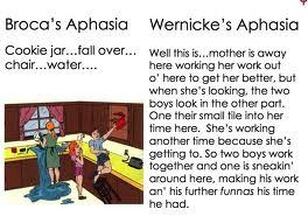
Here is another example of a similar cartoon photo and a response from a patient with Wernicke's aphasia compared to one with Broca's aphasia. Image courtesy of https://aphasia-and-brain-blog.tumblr.com/post/45064637785/examples-of-scenario-description-by-both-brocas
|
Wernicke’s aphasia, a receptive (fluent) aphasia, generally occurs in conjunction with a lesion to the left posterior lobe of the brain. After such lesions, the patient often has difficulty understanding language and/or (depending on the severity) forming meaningful utterances. The speech appears fluent but is often nonsensical. In many cases patients are unaware of their inability to produce intelligible speech and believe that they are speaking normally. This can cause extreme paranoia and anxiety in many individuals (Cummings & Mega, 2003).
Patients with Wernicke’s aphasia will use paraphasias, or incorrect substitutions of words for similar sounding or entirely different words. There are three major categories of paraphasic errors according to the Encyclopedia of Autism Spectrum Disorders, including phonemic paraphasia in which one phoneme is substituted for another (“bog” instead of “dog”), verbal paraphasia in which the person says a completely different word than the word that they mean, and neologistic paraphasia in which more than half of the word is incorrect (“drivelee” instead of “driving”). Phonemic paraphasic speech errors were found in a study by Theron et al. (2009) to be significantly more common in the second language of a late-stage bilingual, a finding that is consistent in the medical practice of Dr. Robert Giombetti, MD. Dr. Giombetti is a neurology specialist at Kindred Hospital of Los Angeles, a long-term care facility that commonly treats bilingual patients from all over the Southern California area. He notes that in his practice it is extremely common for the aphasic patient to struggle with their least-familiar language, sometimes to a point of losing the language altogether. There are many variations of Wernicke's aphasia depending upon the severity of the lesion, with some patients retaining the ability to understand simple sentences but finding themselves lost when attempting to interpret more complex utterances. |
AnomiaAnomic aphasia is a form of aphasia that can be found both within other aphasias and on its own. It is a symptom of many disorders affecting the cerebral hemispheres, and presents itself in three different forms.
|
|
|
|
Global AphasiaGlobal aphasia is a nonfluent aphasia in which a patient struggles with all aspects of language, from producing it to understanding it. The only sounds that global aphasics are able to produce on their own accord are nonsensical, or are repeated stock phrases (“hello” or “I can’t”) (Cummings & Mega, 2003, p. 77). Though oftentimes able to follow total physical response commands and able to distinguish their native language from others, global aphasics are almost entirely unable to produce original utterances. These patients can almost never read or write following their trauma. This generally results from a severe injury to the entire left hemisphere, damaging almost all areas of functional linguistic communication including Broca’s and Wernicke’s areas.
|
Bilingual Aphasia
There is no one specific language outcome in bilinguals who suffer from aphasia due to brain trauma. The end result depends upon the same specific variables as those of patients with all disorders related to traumatic brain injury (see "Variables Affecting TBI Language Deficit Severity"). Yet even when taking these variables into account, most cases of bilingual aphasia are extremely differential.
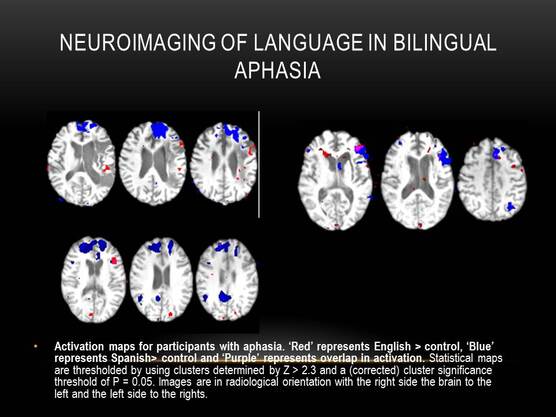
Image courtesy of Boston University. This neuroimaging scan displays areas where each language of a bilingual is being processed and where the two languages overlap.
This differential response across bilinguals supports the theory that bilingual language centers may exist on either side of the brain (see “The Debate of Lateralization”); if there were one expected outcome, for example a loss of both languages with a left-hemispheric lesion, it could be assumed that only one hemisphere controls language. However, because there are a variety of possible outcomes, it is likely that the individual brains of bilinguals have a unique composition of language depending upon age of acquisition, level of fluency, how often the language is used, among an assortment of variables. This is best explained by Michel Paradis' (2001) theory of bilingual aphasia, centered around his "Subset Hypothesis,": though some of the bilingual's language centers coincide, there are also subsets of language that are separated and can be found in different parts of the brain (p. 9). This places some language processing centers in some bilinguals in the non-dominant hemisphere.
It is extremely rare for a bilingual person to have equal fluency in both languages; generally there is one language that the patient considers "dominant" to the other. With the diagnosis of aphasia, the dominance of each language comes into conjunction with the location of the lesion to form unique aphasic symptoms. The languages may recover in parallel, or may become disjoint and non-parallel with one language recovering more significantly than the other.
Bilingualism does not increase the individual’s susceptibility to aphasia. There is also no evidence that bilinguals with aphasia take significantly longer to recover the use of one or both languages than monolingual individuals. However, the level of language impairment in aphasia that occurs in both languages may influence verbal fluency, similar to the way that it does in monolinguals.
It is extremely rare for a bilingual person to have equal fluency in both languages; generally there is one language that the patient considers "dominant" to the other. With the diagnosis of aphasia, the dominance of each language comes into conjunction with the location of the lesion to form unique aphasic symptoms. The languages may recover in parallel, or may become disjoint and non-parallel with one language recovering more significantly than the other.
Bilingualism does not increase the individual’s susceptibility to aphasia. There is also no evidence that bilinguals with aphasia take significantly longer to recover the use of one or both languages than monolingual individuals. However, the level of language impairment in aphasia that occurs in both languages may influence verbal fluency, similar to the way that it does in monolinguals.
