The Bilingual Brain After TBI
|
The culmination of increased cognitive function and potential bilateralization results in a generally favorable recovery outcome for bilingual patients with TBI. However, a bilingual individual is just as susceptible to brain damage as a monolingual individual, and immediately after injury there are a myriad of deficits that these patients can acquire just as easily as monolingual patients, including changes in mood, extreme fatigue, difficulty with memory, and even paralysis. A bilingual's ability to switch languages may also be impaired accompanying frontal lobe injury, along with any possible speech disorders. Therapies dealing with this specifically will be discussed in "Diagnosis & Treatment."
|
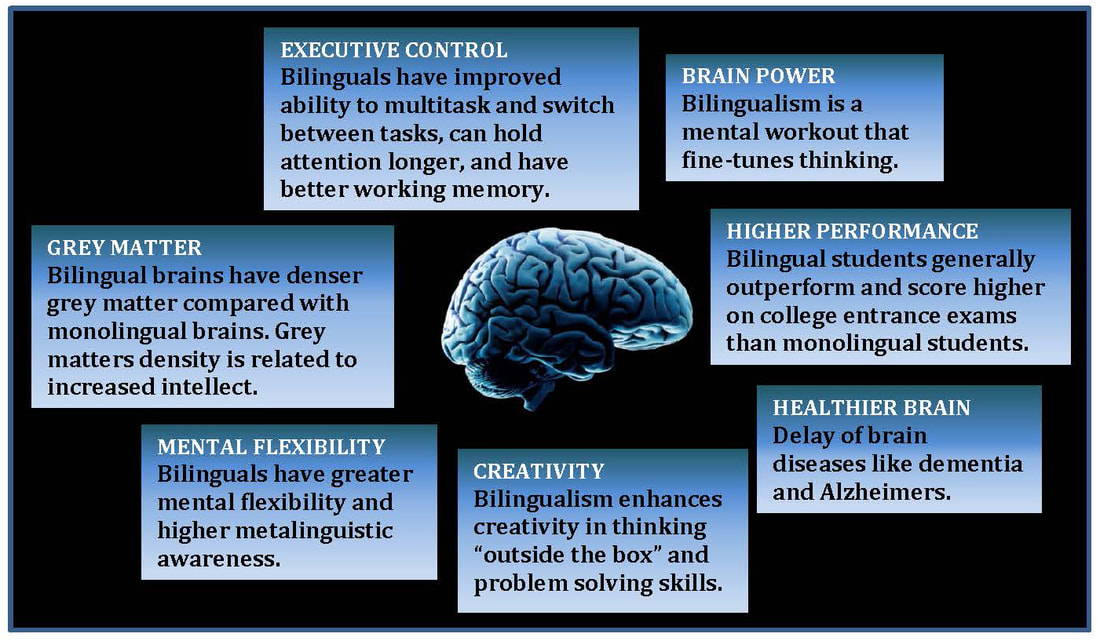
Some of the many benefits of a bilingual brain, many of which can result in a more favorable outcome for language recovery after traumatic brain injury. Image courtesy of DePaul University College of Education
|
Immediately following an injury, however, bilinguals theoretically have an increased likelihood of developing language impairments. If their linguistic lateralization is similar to that of individuals who are cerebrally ambilateral--which would be a logical assumption considering evidence of bilingual bilateral language distribution (see "The Debate of Lateralization")--then many bilingual individuals will have language processing and production centers stored in both hemispheres, which increases the likelihood that injury to any hemisphere will cause speech or language disorder. As this increase in risk is often observed in patients who are cerebrally ambilateral, who often develop deficits in language regardless of the hemisphere that is injured, it can be assumed that cerebrally ambilateral bilinguals will respond similarly (Cummings & Mega, 2003, p. 74).
However, if this increases patient exposure to language deficit after trauma, the same factors will allow for an increased rate of recovery. Because language is stored in both hemispheres in many cases, the opposing hemisphere will be able to compensate for the language deficit in the lesioned hemisphere. Therapy in one of the bilingual patient's languages has been observed to increase language ability in the other language as well, thus allowing the patient to utilize the surviving language in therapy in order to reclaim the lost language (Ansaldo & Saidi, 2014, p. 3; Knoph, Simonsen, & Lind, 2017, p. 1483). Due to this common phenomenon of simultaneous recovery, there is no evidence that the average bilingual patient has more difficulty recovering from brain trauma than the average monolingual patient.
However, if this increases patient exposure to language deficit after trauma, the same factors will allow for an increased rate of recovery. Because language is stored in both hemispheres in many cases, the opposing hemisphere will be able to compensate for the language deficit in the lesioned hemisphere. Therapy in one of the bilingual patient's languages has been observed to increase language ability in the other language as well, thus allowing the patient to utilize the surviving language in therapy in order to reclaim the lost language (Ansaldo & Saidi, 2014, p. 3; Knoph, Simonsen, & Lind, 2017, p. 1483). Due to this common phenomenon of simultaneous recovery, there is no evidence that the average bilingual patient has more difficulty recovering from brain trauma than the average monolingual patient.
Variables Affecting TBI Language Deficit Severity
Many doctors and speech therapists more commonly witness a deficit in the patient’s second language than in their first language after TBI, especially if that language was learned after the critical age period. The speaker’s first language is more likely to be more automatic and familiar due to method and age of acquisition, as this is the language that was most likely acquired instead of learned. Dr. Robert Giombetti, MD, of Kindred Hospital Los Angeles has seen many more cases of individuals losing their second language after traumatic brain injury than losing their first, and notes that first language loss and second language endurance is rare in his practice (personal interview, 2020).
There are multiple possible explanation for language loss or depletion due to traumatic brain injury. Though common, there are a variety of variables that account for which of a bilingual’s languages is the most easily recovered or preserved after TBI. These variables are listed below.
There are multiple possible explanation for language loss or depletion due to traumatic brain injury. Though common, there are a variety of variables that account for which of a bilingual’s languages is the most easily recovered or preserved after TBI. These variables are listed below.
- The language that is the most "familiar": this variable can be attributed to many of the other variables in this list. For example, the most "familiar" language could also be the one that was learned first and stored almost entirely in the left side of the brain, and could also be the language used most in daily life. "Familiarity" is subjective and based in itself upon a variety of variables, most of which are already listed here.
- The order in which the language was learned: the first language will be acquired instead of learned, and the subject will have native speaker fluency.
- The language that is the most “automatic”: generally this is the first language, but in many cases, over a long period of time a person’s dominant language can change, especially if their environment changes. For example, a young boy who moves to America from China may have learned Mandarin Chinese as his first language. He learned English in kindergarten, and now speaks English more often than Mandarin Chinese.
- The language with the strongest emotional association
- The language used most in daily life
- The language that the patient can read and write in
- The language “of the clinical environment and of therapy delivery”: Speech pathologist Lea Treworgy almost always conducts her initial assessments of TBI patients in the patient’s first language, and, because the majority of her patients are Spanish-English bilinguals, uses both languages to communicate with the patient and their family (Lorch, 2014, p. 106).
There is no one outcome to expect from the speech of a post-TBI bilingual individual, so to ensure that both the family and the patient are well aware of the implications of the patient's illness it is imperative that communication be available to the client and the family in both languages. Not only does this allow for better understanding and rapport between the speech therapist and the patient, but the amount of background information that is able to be provided by the bilingual patient about their condition has been shown to increase dramatically with bilingual communication (Foster, 1992, p. 474). All speech therapy should be prepared to use a language other than English to conduct interviews, assessments, and even therapy itself in order to best treat bilingual patients.
Bilingual TBI & the Healthcare System
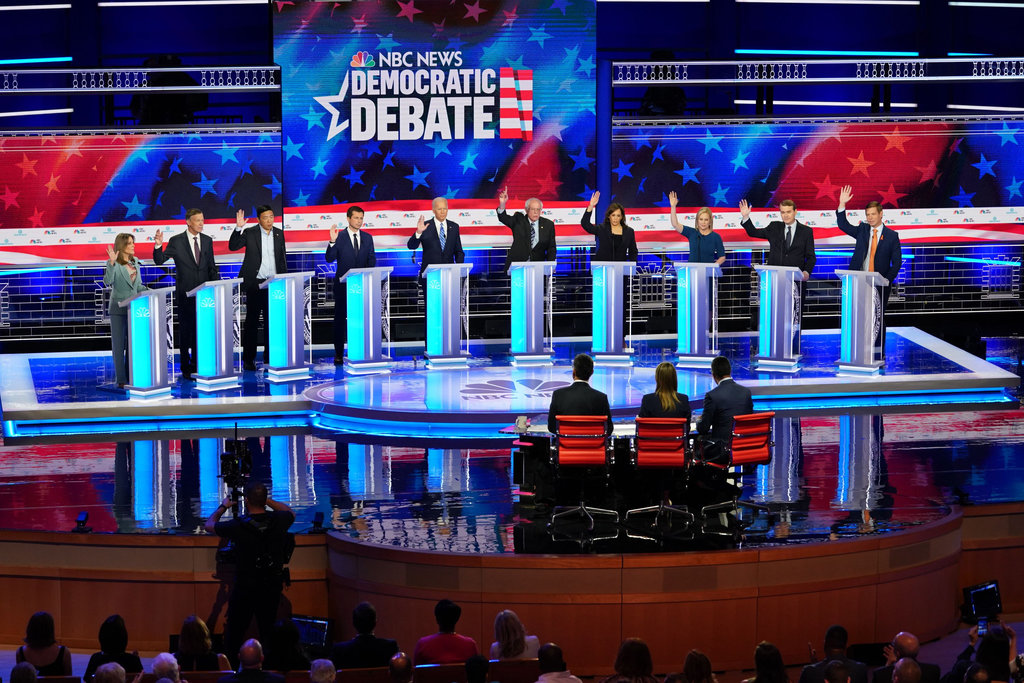
Candidates during the 2020 Democratic Debate pledging to provide healthcare for undocumented immigrants. Image courtesy of the New York Times.
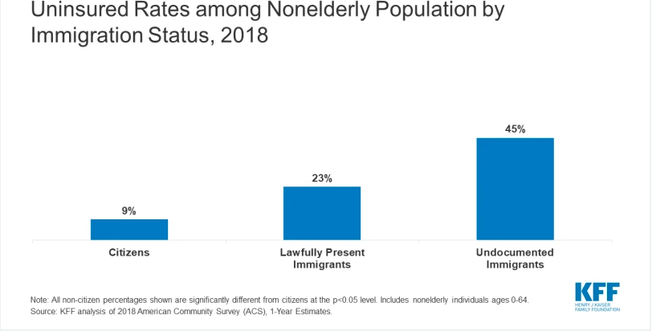 Image courtesy of the Henry J Kaiser Family Foundation
Image courtesy of the Henry J Kaiser Family Foundation
Though evidence points to more favorable cognitive conditions in bilinguals than in monolinguals when it comes to language and brain rehabilitation, people of color, who are more likely to be bilingual than White Americans, have been found to be disproportionately at risk of incomplete recovery after traumatic brain injury. Oftentimes this is due to non-biological and generally circumstantial factors, such as poorer quality of and access to healthcare. African-American and Hispanic individuals are significantly less likely to have consistent access to a healthcare provider than a White individual, leading to more untreated cases of traumatic brain injury (Gary, Arango-Lasprilla, Stevens, 2009, p. 779).
High medical bills from TBI also devastate low-income and immigrant families of all backgrounds, with many individuals often plunging deep into debt. Because of this, many individuals suffering from mild to moderate brain injury do not seek medical attention. Yet even with many of these cases of TBI unaccounted for in hospital records, African-Americans and Hispanics still have a significantly higher percentage of TBI cases than White Americans, with 278 injuries per 100,000 people and 262 per 100,000 people respectively, in comparison to White Americans who account for 209 per 100,000 (Gary, Arango-Lasprilla, Stevens, 2009, p. 780). Hispanics and Blacks are also twice as likely than Whites to be discharged from hospitals after traumatic brain injury instead of sent to a long-term care facility where more care can be provided (Chang et al., 2008, as cited by Gary, Arango-Lasprilla, and Stevens, 2009, p. 780). This lack of critical care often decreases the cognitive recovery advantage that bilinguals enjoy and favors privileged White individuals, most of whom are monolingual.
Immigrant populations are the least likely to have healthcare and the most likely to be bilingual, with 33 percent of the United States immigrant population reporting to have no access to healthcare (about half of this population being undocumented) and 15 percent obtaining basic access to healthcare through Medicare and Medicaid (Bustamante & Van der Wees, 2012). As traumatic brain injury generally requires an extended hospital stay, most undocumented individuals are unlikely to subject themselves to high fees and the possibility of deportation that comes with treatment. Undocumented individuals are also more likely to work physically demanding jobs, increasing their likelihood for traumatic injury (tbionthehill, 2018). In all, this population is most at risk for adverse effects of TBI regardless of the cognitive benefits that bilingualism provides.
Disparate access to healthcare is the main detractor toward bilingual recovery, and one of the leading causes for gaps in recovery research. Though bilingual brains are able to recover language through increased white matter connections and bilaterality, these individuals are unable to reap those benefits if they are not given the same treatment as more commonly monolingual White individuals.
High medical bills from TBI also devastate low-income and immigrant families of all backgrounds, with many individuals often plunging deep into debt. Because of this, many individuals suffering from mild to moderate brain injury do not seek medical attention. Yet even with many of these cases of TBI unaccounted for in hospital records, African-Americans and Hispanics still have a significantly higher percentage of TBI cases than White Americans, with 278 injuries per 100,000 people and 262 per 100,000 people respectively, in comparison to White Americans who account for 209 per 100,000 (Gary, Arango-Lasprilla, Stevens, 2009, p. 780). Hispanics and Blacks are also twice as likely than Whites to be discharged from hospitals after traumatic brain injury instead of sent to a long-term care facility where more care can be provided (Chang et al., 2008, as cited by Gary, Arango-Lasprilla, and Stevens, 2009, p. 780). This lack of critical care often decreases the cognitive recovery advantage that bilinguals enjoy and favors privileged White individuals, most of whom are monolingual.
Immigrant populations are the least likely to have healthcare and the most likely to be bilingual, with 33 percent of the United States immigrant population reporting to have no access to healthcare (about half of this population being undocumented) and 15 percent obtaining basic access to healthcare through Medicare and Medicaid (Bustamante & Van der Wees, 2012). As traumatic brain injury generally requires an extended hospital stay, most undocumented individuals are unlikely to subject themselves to high fees and the possibility of deportation that comes with treatment. Undocumented individuals are also more likely to work physically demanding jobs, increasing their likelihood for traumatic injury (tbionthehill, 2018). In all, this population is most at risk for adverse effects of TBI regardless of the cognitive benefits that bilingualism provides.
Disparate access to healthcare is the main detractor toward bilingual recovery, and one of the leading causes for gaps in recovery research. Though bilingual brains are able to recover language through increased white matter connections and bilaterality, these individuals are unable to reap those benefits if they are not given the same treatment as more commonly monolingual White individuals.
|
|
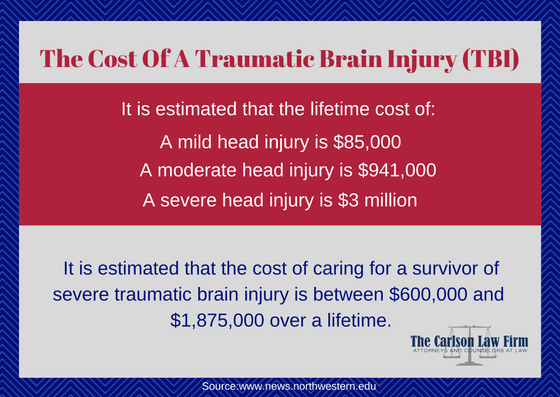
The monetary costs of TBI. Image courtesy of Carlson Law Firms
|
