Diagnosis
|
Diagnostic assessments are conducted before the onset of therapy in order to gauge the severity of language deficit after TBI. When working with bilingual patients, these are conducted in both the individual's first and second languages. Speech-language pathologist Lea Treworgy begins the assessment by interviewing the family (generally in the family's first language in order to obtain as much information as possible) about the patient's medical history. Oftentimes, she conducts the assessment in both the individual's first and second language in order to discern whether or not the speech disorder affects both languages.
The assessment consists of an initial determination of language output, with disfluent speakers exhibiting significantly less verbal output than normal (10-50 words per minute) and fluent speakers displaying normal or increased verbal output (200+ words per minute) but often with decreased evidence of contextual or sensical utterances. Motor skills are also assessed, with productive linguistic motor skills associated with an intact Broca's area. The speech pathologist then conducts an assessment of language comprehension. This includes semantic tests of increasing complexity that are able to determine the severity of language deficit in the patient. These involve a variety of contexts including social, educational, and vocational settings (American Speech-Language-Hearing Association, 2020). This yields information about how severely the Wernicke's area and surrounding brain areas are affected (generally in a posterior lesion). The patient's ability to repeat sounds, words, and phrases is also tested. If the patient is unable to repeat these, especially in forms of Broca's and Wernicke's aphasias, they substitute paraphasias for the repeat phrases. Injuries that result in difficulty with this kind of repetition often stem from damage to areas near the sylvian fissure (Cummings & Mega, 2003, p. 75). Most speech pathologists who are not bilingual use translators during assessment and many other parts of therapy in order to create an accurate depiction of the individual's language ability. Bilingual evaluations are also available and easy to find in both languages. |
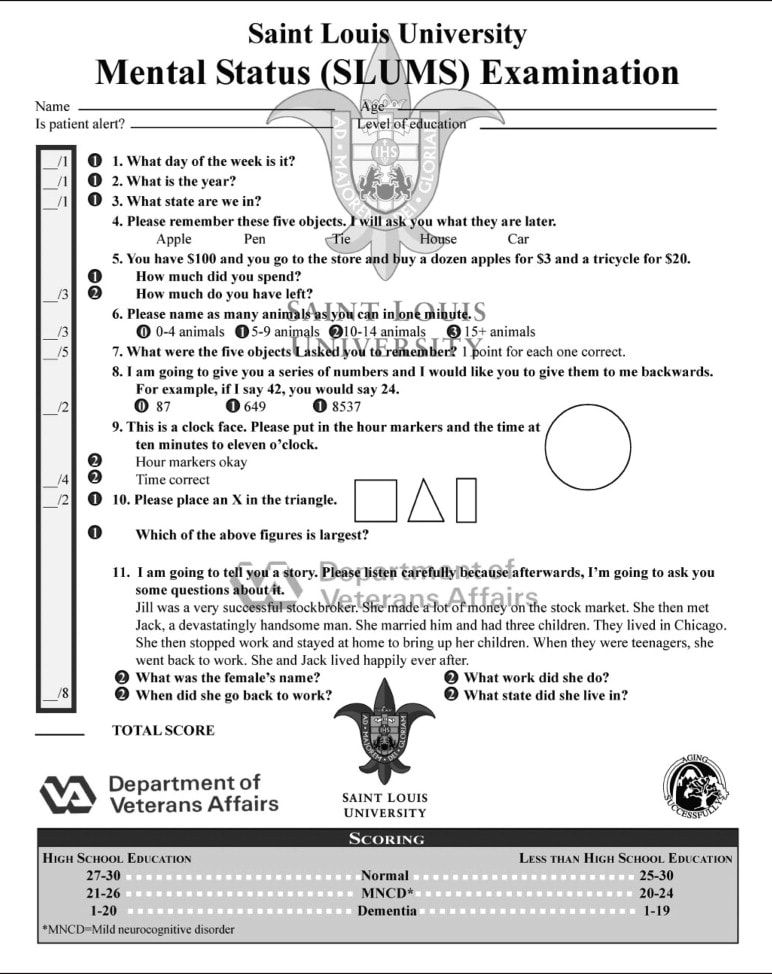
The Saint Louis University Mental Status Examination, an assessment usually given to patients following TBI. Available in multiple languages for bilinguals. Image courtesy of Tariq et al. (2006).
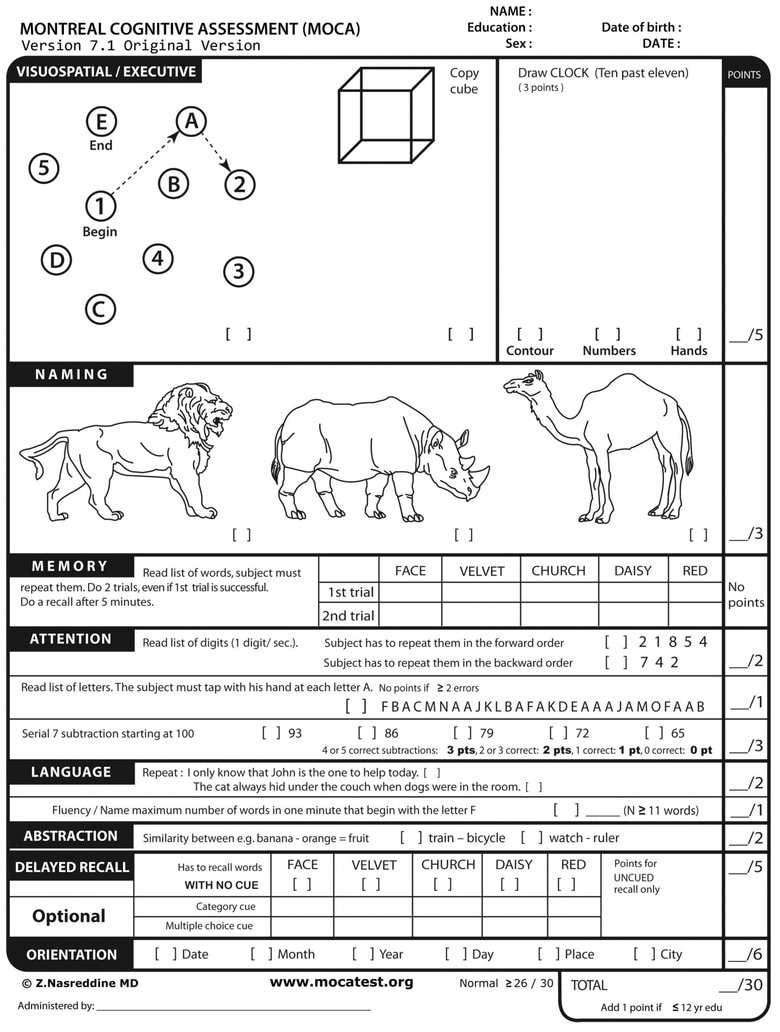
The Montreal Cognitive Assessment, another assessment given to patients after TBI and also available in multiple languages. Image courtesy of The Seattle Times.
|
Treatment
The language of treatment depends upon the language that is most affected by the lesion. Most SLPs conduct therapy in the native language, due to evidence that progress made in the native language usually transfers to the second language (Marangolo & Rizzi, 2009, p. 406; Ansaldo & Saidi, 2014, p. 8). However, in other cases, treating the less dominant language specifically has resulted in the largest percent of linguistic transfer between both of the injured patient's languages (Ansaldo & Saidi, 2014, p. 8)
Treatment itself also depends upon the severity and location of the lesion. It generally begins slowly, allowing time for the brain to heal initially from the wound. In the videos below, a professor and a speech-language pathologist give examples of possible methods of TBI treatment.
Treatment itself also depends upon the severity and location of the lesion. It generally begins slowly, allowing time for the brain to heal initially from the wound. In the videos below, a professor and a speech-language pathologist give examples of possible methods of TBI treatment.
|
|
Treatment involves
|
Hemispheric Compensation & Linguistic Transfer
In recovery of traumatic brain injury, many researchers have found evidence of a link between recovery in the bilingual individual’s first language and recovery in their second language. Connections such as the understanding of cognates allow for the transfer of linguistic knowledge from one language to another, so that therapy in one language leads to the same recovery in the other. Evidence of cognate transfer is also evidence of strong connections between the L1 and the L2 in the brain, and corroboration to the theory that bilingual individuals are not stifled in their recovery because of another language. The historic belief that bilinguals have a more difficult time recovering from brain injury because they must relearn both languages is demonstrated to be purely mythical.
This coincides with the theory of hemispheric lateralization, and with evidence of increased right hemisphere involvement in language and other dominant-hemispheric tasks during a left-hemispheric lesion. Thiel et. al (2001) found that, in a patient whose left hemisphere was infected with tumors, the right hemisphere demonstrated evidence of basic linguistic competency, a finding that has been supported by Basso et al. (1989); Heiss, Kessler, Thiel, Ghaemi, & Karbe (1999); Ohyama et al. (1996); Raboyeau et al. (2008); Saur et al. (2006); and Winhuisen et al. (2005). The right hemisphere's ability to compensate for the left hemisphere's deficits supports the idea that the utilization of language stored in the contralesional hemisphere through therapy can assist in rehabilitation of a patient's fluency.
This coincides with the theory of hemispheric lateralization, and with evidence of increased right hemisphere involvement in language and other dominant-hemispheric tasks during a left-hemispheric lesion. Thiel et. al (2001) found that, in a patient whose left hemisphere was infected with tumors, the right hemisphere demonstrated evidence of basic linguistic competency, a finding that has been supported by Basso et al. (1989); Heiss, Kessler, Thiel, Ghaemi, & Karbe (1999); Ohyama et al. (1996); Raboyeau et al. (2008); Saur et al. (2006); and Winhuisen et al. (2005). The right hemisphere's ability to compensate for the left hemisphere's deficits supports the idea that the utilization of language stored in the contralesional hemisphere through therapy can assist in rehabilitation of a patient's fluency.
Cross-Linguistic Transfer Therapy
|
As mentioned in previous sections, bilinguals with TBI can have difficulties with language control, or the ability to switch from one language to another, especially if there is a lesion to the frontal lobe of the brain (Ratiu & Azuma, 2017, p. 29). Although this may seem to put bilinguals at a disadvantage to monolinguals, language control is not specific to bilinguals: monolinguals use language control to assess situational pragmatics as well as to change register (Anderson et al., 2018, p. 352). Because of their use of language control within all of these parameters, bilinguals have been observed to have more refined systems of control, resulting in an increased ability to multitask and switching fluently between two assignments (Park-Johnson, 2016). Simultaneous recovery is expected in bilinguals with language control difficulties, indicating that knowledge of two languages does not designate significant disadvantage to recovery (Green & Abutalebi, 2008, p. 568). Both bilinguals and monolinguals with language control problems will require additional therapy in order to restore these previous skills.
|
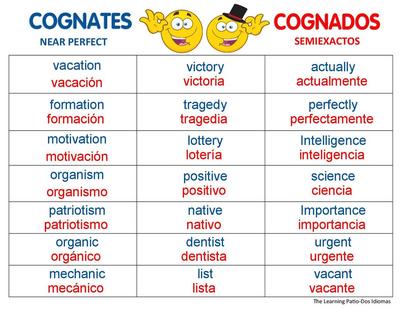
Cognates between English and Spanish. Image courtesy of https://quizizz.com/admin/quiz/5da5f9d99c3aec001afcd106/spanish-cognates
|
Through methods such as cross-linguistic transfer, bilinguals are able to make connections between their first and second languages in order to heal the ability of language control. According to Ansaldo & Saidi (2014), therapy focused upon the weaker language in this scenario has been demonstrated to transfer more effectively across the multiple languages spoken by the patient. Using this less proficient language--one that may be stored in the non-dominant, non-lesioned hemisphere--therapists are able to recover both languages. Because languages can recover in tandem this way, there is evidence that the knowledge of an additional language does not necessarily mean that there is more therapy necessary than a monolingual with issues of language control, or that the bilingual individual is at a disadvantage during recovery. Through cross-linguistic language therapy (CLT), bilingual individuals are able to reacquire language control and use it to rehabilitate both languages.
CLT is conducted initially using cognates between the individual's first and second languages. The distance between language families (the amount of similarities and differences between families of languages) is often taken into account here, as well as the proficiency in both languages before and after the lesion. In brain-damaged patients, cognates are processed as efficiently as in the native language, which allows for transfer of meaning between the understood language and the lost language (Anton-Menendez & Gollan, 2010, as cited by Ansaldo & Saidi, 2014, p. 3). Lexical retrieval strategies such as cueing, and word association and recognition were employed to assist the patient in connecting the cognates.
CLT is conducted initially using cognates between the individual's first and second languages. The distance between language families (the amount of similarities and differences between families of languages) is often taken into account here, as well as the proficiency in both languages before and after the lesion. In brain-damaged patients, cognates are processed as efficiently as in the native language, which allows for transfer of meaning between the understood language and the lost language (Anton-Menendez & Gollan, 2010, as cited by Ansaldo & Saidi, 2014, p. 3). Lexical retrieval strategies such as cueing, and word association and recognition were employed to assist the patient in connecting the cognates.
Recovery
|
In 1987, Michel Paradis outlined six major patterns of recovery of speech in instances of traumatic brain injury. Specifically these patterns of recovery refer to aphasia caused by TBI, but can also refer to other speech impairments caused by TBI. Today these are divided mostly into “parallel” and “nonparallel” forms of recovery.
Parallel & Nonparallel |
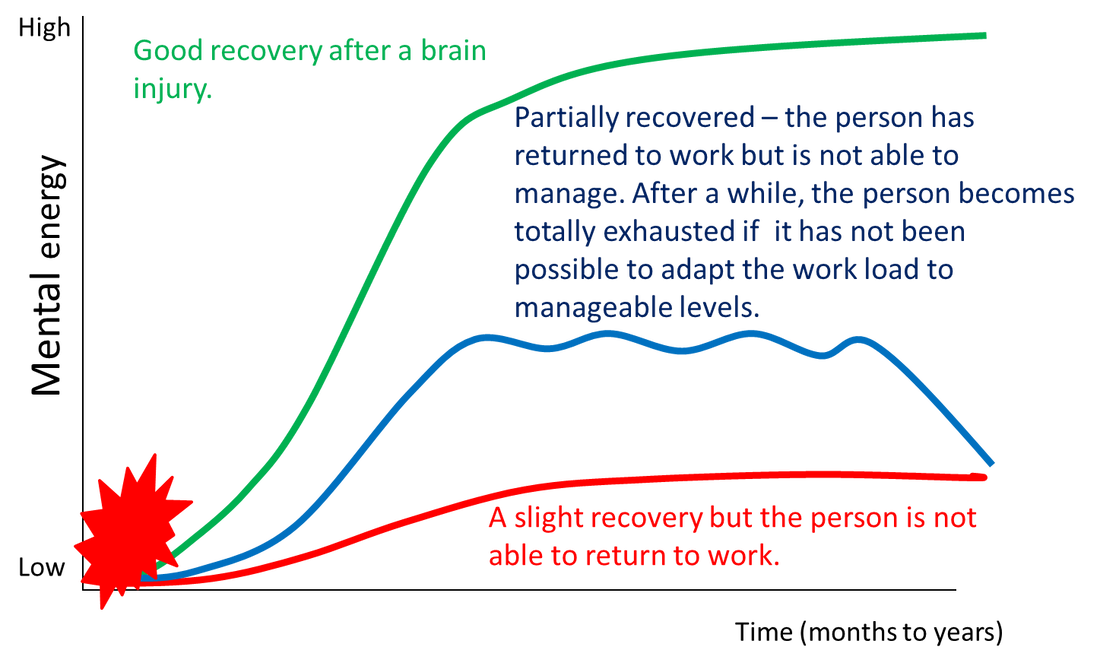
Though "good," "partial," and "incomplete" recovery generally refers to overall cognitive function of an individual after a TBI, language consists of a significant portion of that. Without ability to produce or comprehend fluent language, the patient would be unable to return to work or school. Image courtesy of https://www.intechopen.com/books/traumatic-brain-injury/long-lasting-mental-fatigue-after-traumatic-brain-injury-a-major-problem-most-often-neglected-diagno
|
- parallel recovery: in parallel recovery, one language appears to recover in tandem with the other. Most forms of therapy are conducted specifically in one of the individual’s two languages and the progress that is made to one most often transfers to the other (Marangolo & Rizzi, 2009, p. 406; Ansaldo & Saidi, 2014, p. 8). This is made easier by cognates between each of the individual’s languages (Ansaldo & Saidi, 2014, p. 8). When language control is not an issue, parallel recovery is generally expected (Marangolo & Rizzi, 2009, p. 406; Ratiu & Azuma, 2017, p. 37). (Loss of language control is generally associated with frontal lobe lesions and results in the inability to switch between first and second languages). Evidence of parallel recovery supports the theory that the right hemisphere can compensate for language deficits in the left hemisphere after traumatic brain injury, especially when the right hemisphere contains more areas of language processing than strictly left-brained language dominant individuals (i.e bilinguals or the cerebrally ambilateral) (Marini et. al, 2016, p. 41).
- nonparallel recovery: the variables that affect severity of language deficit in TBI also affect the rate of recovery (see “Variables Affecting TBI Language Deficit Severity”). The variable that affects recovery the most is familiarity of language, regardless of whether or not the language was the first that the patient learned (Obler, 1977, p. 467).
- selective recovery: the language that is most familiar to the patient recovers first
- successive recovery: one language recovers fully and the other is inaccessible
- differential recovery: one language, regardless of what language it is, is more affected than the other
- antagonistic recovery: one language recovers while the other degenerates
- mixed recovery: seen when the patient has difficulty distinguishing between the two languages, failing to inhibit one language in order to speak the other
The greatest amount of recovery occurs within the first 3-6 months of therapy, continuing on in fewer and fewer amounts for the next five years. Young patients are able to recover language use at a higher rate than older patients, and left-handed patients are more likely to recover than right-handed patients (Cummings & Mega, 2003, p. 83). The favorable conditions that left-handed individuals have is in part due to their opposing lateralization and the increased likelihood that they have stored language in both hemispheres of their brain similarly to bilinguals. This evidence supports the theory that cerebrally ambilateral individuals, including bilinguals, are biologically dispositioned to more favorable outcomes after TBI.
Rita's Story
 Rita on the cover of the American Speech-Language-Hearing Association newsletter in October, 2016.
Rita on the cover of the American Speech-Language-Hearing Association newsletter in October, 2016.
68-year-old "Rita" was born in Venezuela and moved to New York City when she was 32. She has been bilingual in English and Spanish for most of her life, but after suffering a stroke that caused traumatic brain injury to the left side of her brain, she struggles with both languages. She relies most heavily upon Spanish, her first language, but has generally preserved comprehension in both languages, and most likely suffers from Broca's aphasia.
Bilingual clinicians interviewed Rita and her family about Rita's language background (which language she learned first, how long she had been speaking them, which she uses more often, etc.). An aphasia assessment was then conducted in English and in Spanish to determine the extent of Rita's aphasia. Treatment centered around direct translation from Spanish to English proved effective in the recovery of Rita's English ability. Rita and her therapists also practiced cross-linguistic transfer, which proved to be extremely effective (Ansaldo & Saidi, 2014, p. 3). She has shown consistent progress in regaining fluency of both languages, a promising outcome for other similar bilingual patients.
Bilingual clinicians interviewed Rita and her family about Rita's language background (which language she learned first, how long she had been speaking them, which she uses more often, etc.). An aphasia assessment was then conducted in English and in Spanish to determine the extent of Rita's aphasia. Treatment centered around direct translation from Spanish to English proved effective in the recovery of Rita's English ability. Rita and her therapists also practiced cross-linguistic transfer, which proved to be extremely effective (Ansaldo & Saidi, 2014, p. 3). She has shown consistent progress in regaining fluency of both languages, a promising outcome for other similar bilingual patients.

Rita. Image courtesy of https://leader.pubs.asha.org/doi/10.1044/leader.FTR2.21102016.52
